Fertility, pregnancy, and plastic exposure
What the science suggests
Plastic is easy to mistake for a single thing. A bottle. A lid. A food container. A material that seems stable because it holds its shape.
But biologically, plastic is rarely encountered that way.
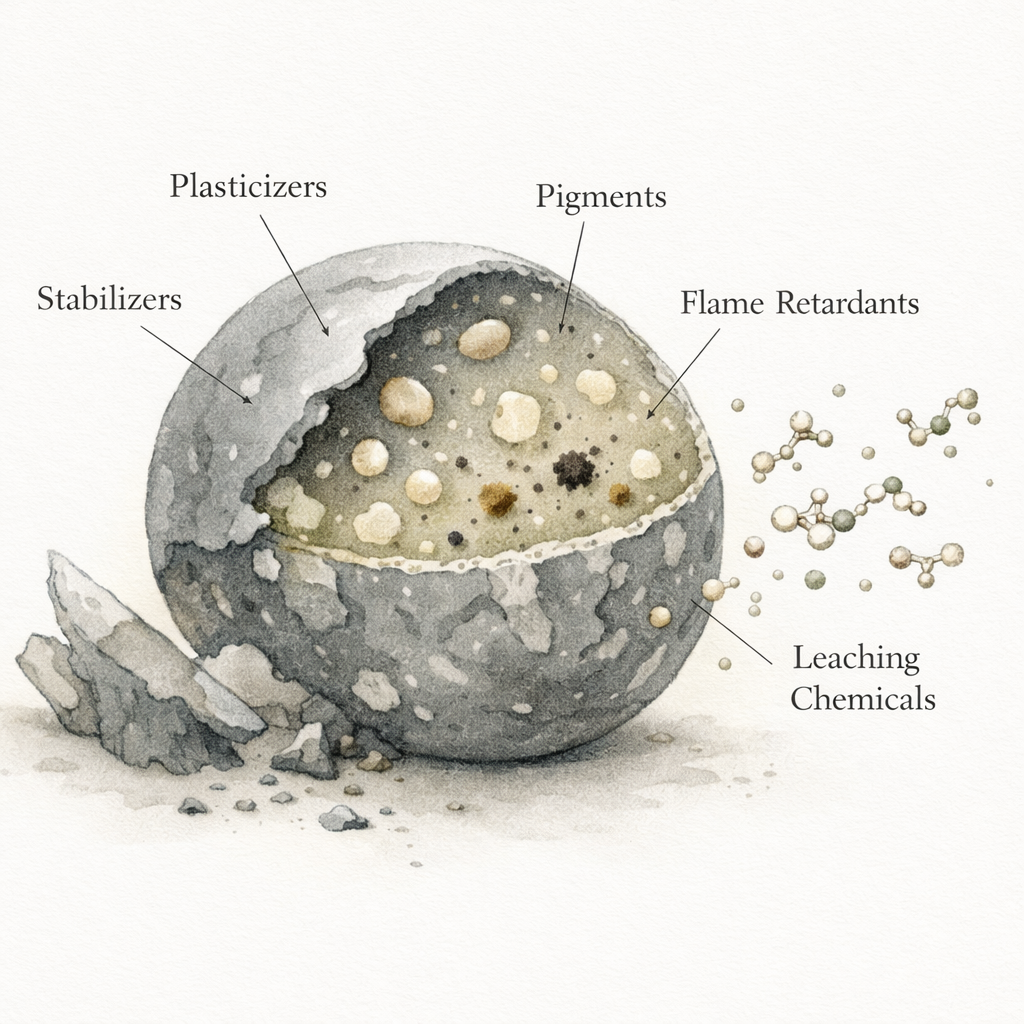
Most plastics are engineered blends. A base polymer is combined with additives that give the finished material its useful properties. Plasticizes improve flexibility. Stabilizers slow degradation. Pigments add color. Flame retardants improve safety and performance. What we call “plastic” is often less like one inert substance and more like a functional chemical system.
Over time, that system changes. Additives can leach. Larger materials can fragment into smaller particles. Those particles can carry traces of the chemicals used to make them, along with contaminants absorbed from the surrounding environment. In practice, the body does not encounter plastic as one exposure. It encounters a complex and changing mixture of particles, additives, and associated pollutants.
That matters in every organ system. But it may matter especially in reproduction and development.
Reproductive biology is exacting. Fertility depends on tightly timed hormone signals, healthy mitochondrial function, intact barrier structures, and carefully regulated immune tolerance. Pregnancy adds another layer of precision. The placenta must nourish and protect at the same time. Development depends on sequence, timing, and cellular communication unfolding with remarkable consistency. In systems like these, even subtle interference can matter.
The central question is no longer whether plastic related exposures can reach reproductive systems. A growing body of human evidence suggests they can. The more important question now is how those exposures interact with fertility, pregnancy, and development, and how confidently the science allows us to interpret the signals we are beginning to see.
Plastic exposure is a mixture problem
One reason this field is difficult to interpret is that “plastic exposure” is not one exposure.
It may involve particles of different sizes, shapes, and polymer types, from larger microplastics down to nanoplastics small enough to behave differently in tissues. It may also involve plastic associated chemicals such as phthalates and bisphenols, compounds with their own reproductive and endocrine literature. In addition, plastics can adsorb other contaminants from the environment they move through.
This means the biological story is unlikely to revolve around a single mechanism. It is more plausible that reproductive risk, where it exists, reflects a layered interaction involving particle transport, oxidative stress, inflammation, endocrine disruption, mitochondrial injury, and barrier dysfunction. This one one reason the literature can feel fragmented at first. Different studies are often measuring different parts of the same broader exposure system.
Seen this way, the field becomes easier to read. The question is not whether one isolated plastic particle causes one isolated reproductive outcome. The question is whether a blend class of exposures is beginning to leave a detectable signature in reproductive biology.
Human studies are beginning to detect plastics where reproduction happens
The most important shift in this field is simple. Human studies are no longer discussing reproductive exposure as a distant possibility. They are beginning to measure plastic particles in the tissues and fluids where reproduction and development actually occur.
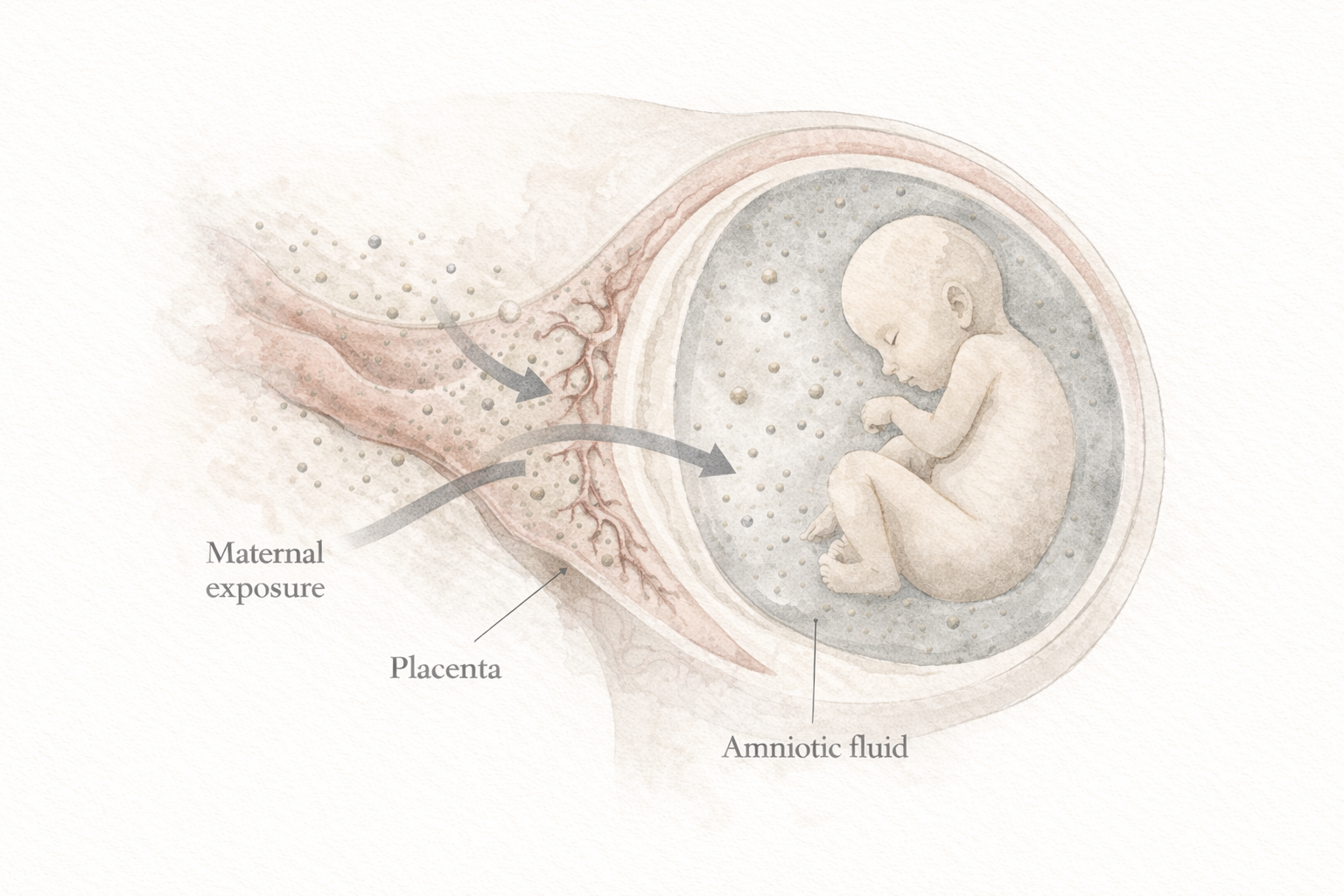
The placenta has become one of the clearest examples. As the interface between maternal and fetal physiology, it regulates nutrient transfer, immune signaling, and protection during pregnancy. In a study of forty three (43) women [[ LINK ]], researchers detected microplastics in all thirteen (13) placentas from pregnancies complicated by intrauterine growth restriction, compared with only three (3) out of thirty (30) placentas from normal pregnancies. The polymers identified included polyethylene terephthalate (PET), polypropylene (PP), polyethylene (PE), and polystyrene (PS). This does not prove that microplastics caused impaired fetal growth. But it does show that plastic particles can appear in placental tissue, and their presence may track with pregnancies already under strain.
That finding does not stand alone. In another placental cohort [[ LINK ]], microplastics were detected in thirty one (31) out of fifty (50) placentas, including polytetrafluoroethylene (PTFE) and acrylonitrile butadiene styrene (ABS). In that study, no adverse outcomes were reported. That contrast matters. It reminds us that detection alone does not equal noticeable harm, and that not every positive finding should be read as evidence of direct injury. At the same time, repeated placental detection changes the baseline conversation. The placenta is not supposed to be a casual repository for synthetic particles.
The fetal environment itself has also entered the picture. In one study of forty (40) pregnancies [[ LINK ]], research found microplastics in thirty two amniotic fluid samples. The polymers included PE, chlorinated polyethylene (CPE), ethylene-vinyl acetate (EVA), styrene-butadiene-styrene (SBS), PET, and polyvinyl chloride (PVC). Higher levels were associated with shorter gestational age. Again, this is observational research. It cannot tell us whether the particles directly contributed to earlier delivery. But it does show that plastics and the chemicals or contaminants they carry may be reaching spaces central to fetal development.
Beyond pregnancy, microplastics are also being detected in reproductive tissues themselves [[ LINK ]]. A study of one hundred sixty (160) women found higher concentrations of microplastics in uterine fibroid tissue than in healthy uterine tissue. The detected polymers included PE, PP, PS, polyurethane (PU), polyethylene vinyl acetate (PEVA), polyphenylene sulfide (PPS), polyacrylonitrile (PAN), PVC, and PET. It is too early to say whether those particles contribute to fibroid formation or preferentially accumulate in tissue that is already diseased. But their presence suggests that reproductive organs may not simply be bypassed by environmental plastic exposure.
Male reproductive health is now showing similar patterns. In a cohort of one hundred thirty one (131) men, microplastics including PS, polycarbonate (PC), PE, PVC, PTFE, PET, and ABS were associated with reduced sperm count and poorer semen quality [[ LINK ]]. Another study of one hundred and thirty three (133) men found PTFE in semen samples and reported reduced sperm count and motility [[ LINK ]].
A separate study involving fifty one (51) couples linked PE and PVC exposure to lower fertilization rates, though implantation after fertilization was unaffected [[ LINK ]].
These studies are still early. Sample sizes are modest. Methods vary. Causation is not yet established. But together they point to a meaningful shift. Plastic particles are now being measured across placenta, amniotic fluid, uterus, semen, and fertility related outcomes. The question is no longer whether reproductive exposure is imaginable. It is measurable.
Animal models add biological plausibility
Human studies show presence. Animal models help explain how that presence might matter.
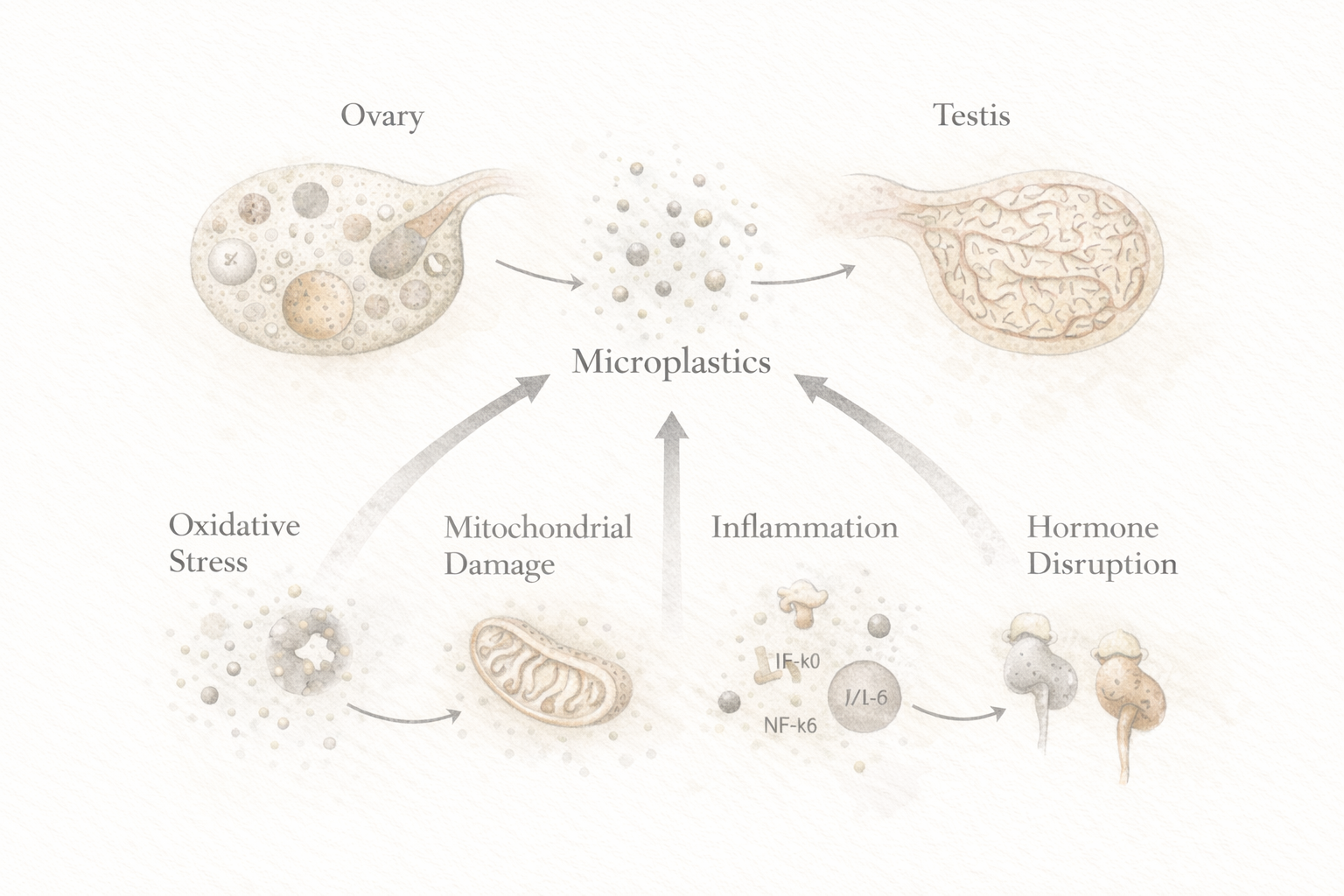
Across rodent and other experimental systems, the signal is remarkably consistent. Researchers repeatedly report disrupted ovarian function, lower ovarian reserve markers, altered estrous cycling, placental dysfunction, impaired sperm production, structural testicular injury, and hormone disruption after exposure to microplastics and nanoplastics. At the cellular level, these changes often converge on the same mechanisms: oxidative stress, inflammatory activation, mitochondrial damage, apoptosis, and endocrine disruption.
In female models, particles have been shown to accumulate in granulosa cells, reduce follicle development, lower anti Mullerian hormone, alter reproductive hormone patterns, and impair oocyte maturation and fertility. During pregnancy, experimental exposure has also been linked to changes in placental metabolism, inflammation, and offspring outcomes, including evidence of transgenerational effects in some models.
Male models mirror this pattern. Studies report reproduced sperm count, lower motility, increased abnormalities, degeneration of seminiferous tubules, disruption of the blood testis barrier, lower testosterone, and accelerated testicular aging. Several papers suggest that mitochondrial injury may be especially important, which is notable because sperm quality relies heavily on energy production and redox balance.
While animal models cannot be mapped directly onto human risk, they offer a useful way to study mechanisms under controlled conditions. By introducing plastic exposures over shorter timeframes and at defined doses, they can reveal biological effects that may help explain what longer term accumulation could do in the real world. Everyday human exposure is more variable and less controlled than laboratory dosing, but the consistency of the mechanistic patterns still matters. Human detection studies show that reproductive tissues can be reached. Animal studies suggest biologically plausible ways those exposures may disrupt reproductive function once they arrive. Cell and culture models then help clarify the underlying biochemistry and molecular pathways involved.
Plastic associated chemicals deepen the story
The reproductive discussion becomes sharper when plastic associated chemicals are considered alongside the particles themselves.
Phthalates, used to make plastics more flexible, have been studied for decades in reproductive toxicology. Human and animal research has linked certain phthalates to lower sperm count and motility, altered testosterone signaling, disrupted ovarian function, and broader developmental effects [[ LINKS ]]. Bisphenol A, used in some plastics and resins, has been associated with altered egg quality, ovarian reserve, implantation related changes, and higher miscarriage risk in some clinical populations [[ LINKS ]].
These two chemicals are often discussed because they are well studies, but they represent only a small part of the additive chemistry used in modern plastics. Many polymers incorporate flame retardants, stabilizers, antioxidants, pigments, and processing aids that can leech out of materials over time.
Brominated flame retardants and new organophosphate flame retardants, for example, are used in plastics and electronic housings and have been linked in some studies to alter hormone signaling and reduced semen quality.
Other compounds may remain as residual monomers from the manufacturing process. Styrene, associated with polystyrene plastics, has been studied for endocrine activity and oxidative stress related toxicity in experimental systems.
Heavy metals, for example cadmium, lead, and chromium, used in plastic stabilizers or acquired from the environment have been shown to act as endocrine disruptors and have known reproductive toxicity.
This does not mean every plastic particle should be interpreted through the lens of BPA or phthalates. It does mean the body is unlikely to be responding to particles alone. Reproductive biology may be responding to a blended exposure landscape in which particles, additives, and other adsorbed compounds interact.
That is the deeper point. Plastic exposure is not just about fragments. It is about the full chemical ecology that travels with them.
Everyday exposure is usually ordinary
For most people, plastic exposure does not begin with an industrial accident or an unusual event. It builds through ordinary routines.
Food and drink are likely major pathways. Bottled water, plastic food packaging, takeout containers, plastic lined lids, synthetic mesh tea bags, and some seafood exposures have all been discussed in the microplastics literature. Infant bottle feeding deserves particular attention because heating and repeated use can release large numbers of particles, while infants carry a higher exposure burden relative to body weight.
Indoor environments matter too. Synthetic textiles shed microfibers. Those fibers accumulate in dust and air and may be inhaled or ingested over time. In practical terms, exposure can begin with very familiar habits: storing hot food in plastic, microwaving plastic containers, drinking from disposable bottles, or living in fiber rich indoor spaces without ever thinking of them as exposure sources.
This does not require panic. It does require perspective. Plastic exposure is ambient. It accumulates gradually through repetition.
What scientists still do not know
This is still an emerging field, and credible interpretation depends on acknowledging its limits.
Most human studies remain observational. Detecting particles in placenta or amniotic fluid does not prove those particles caused a specific complication. A damaged pregnancy may retain more particles for reasons that are not yet clear. Confounding factors may shape both exposure and outcome.
Measurement also remains difficult. Smaller particles are harder to detect, especially nanoplastics. Sampling contamination is a persistent challenge. Different research groups use different methods and reporting standards, which makes comparison across studies imperfect.
Animal data are valuable for understanding mechanism, but laboratory conditions do not fully mirror real life exposure. Humans encounter mixtures across years, not isolated polymers at defined doses. Reproductive health is also shaped by nutrition, metabolic status, smoking, air pollution, occupational exposures, age, infection, and many other variables.
These uncertainties do not erase concern. They define the boundaries of what can be said honestly today.
Why reproduction often acts like an early warning system
Reproductive biology often signals environmental imbalance early because it sits at a particularly sensitive intersection of timing, hormones, mitochondrial health, and barrier function.
Hormone signaling can be disturbed at very low doses. The placenta must simultaneously permit exchange and maintain protection. Eggs and sperm depend on cellular integrity in ways that leave little room for error. When these systems are stressed, the effects may appear first as changes in sperm quality, ovarian reserve, implantation success, placental efficiency, or gestational timing rather than as immediate overt disease.
That is one reason this field matters beyond fertility alone. Reproductive systems can reveal broader environmental strain before other systems make it obvious.
Where the gut fits into the story
For many plastic exposures, the gut is the first meaningful biological interface.
Particles in food, bottled water, salt, and food contact materials typically enter through ingestion. Before reaching the bloodstream, placenta, uterus, or testes, they first encounter the intestinal lumen, mucus layer, microbiota, and gut barrier. That sequence matters. The gut is not just a passageway. It helps determine what remains contained, what interacts locally, and what moves deeper into circulation.
Researchers studying microplastics and the gut are increasingly focused on barrier integrity, inflammatory signaling, microbial shifts, and particle transit. This does not mean the gut is the whole story, or that a gut focused strategy alone resolves reproductive risk. It does suggest that reproductive exposure may begin several biological steps earlier than where it is ultimately detected.
For ingested plastics, the reproductive story and the gut story are linked by sequence.
A measured response
Plastic cannot be removed from modern life overnight. But exposure can often be reduced in practical ways.
Reducing heated food contact with plastic is one of the clearest steps. Glass, ceramic, and stainless steel are often better options for hot food and drinks. Bottled water can be reduced where clean filtered alternatives are available. Plastic rich food contact points such as takeout containers, lined lids, and synthetic tea bags are worth paying more attention to, especially during pregnancy, early childhood, and preconception.
The goal is not purity. It is not fear. It is thoughtful reduction where reduction is feasible.
Conclusion
Plastic exposure is not one thing. It is a layered biological reality made up of particles, additives, and associated contaminants that may interact with sensitive systems in different ways.
In reproductive health, that complexity matters. Human studies now suggest that plastic particles can be detected in placenta, amniotic fluid, uterus, semen, and fertility related settings. Animal studies repeatedly show mechanistic patterns involving oxidative stress, inflammation, mitochondrial injury, and hormone disruption. Decades of work on phthalates and bisphenols add further reason to take the broader exposure landscape seriously.
At the same time, this field is still maturing. Detection does not equal causation. Measurement remains difficult. Real world exposure is mixed and messy. Those uncertainties should make us more precise, not less attentive.
Reproduction is too sensitive, and development is too important, to dismiss these signals simply because the science is still early. The more responsible response is a calm one: keep improving the research, interpret the evidence carefully, and reduce avoidable exposure where practical.
Plastic exposure will not explain every fertility challenge or every pregnancy outcome. But it increasingly belongs in the conversation.